
Hip Clinical Pearls: #14 Derotational Femoral Osteotomy (DFO) |

|
Clinical Pearl #14: The DFO: Derotational Femoral Osteotomy
Just as the PAO is a mouthful of medical terminology, so is the DFO. Neither the PAO or DFO are procedures to laugh about. Both require time and patience throughout the entire process, and thorough diagnosing for assessing if and how if either procedure is for you.
WHAT IS A DFO?
What exactly is a DFO? Why haven't I heard of it before? Why is it recommended for me? In discussing previous procedures, a hip scope alone helps to address bony anatomy issues affecting the joint and fixing the labrum within the joint. The PAO addresses anatomical issues related to poor depth, or formation, of the acetabulum called hip dysplasia. This issue causes an instability within the joint contributing a different presentation of damage within the joint contributing to pain and dysfunction. This was discussed in previous hip pearls. The DFO is a procedure to address the anatomical issues related to the orientation of the femur to the hip socket. In my experience, the number of orthopedists who look for either or both dysplasia and femoral torsion are increasing whereas in the past, these were not as well identified as to how these effected the joint and damage related to labral or cartilage tears. In addition, these are typically not diagnoses which PCPs will be looking for upon an assessment. The hip world continues to change and evolve rapidly, and these statements will hopefully be too old before too long!
Why does this matter? The orientation of the angle of the neck of the femur at the top of the bone compared to the condyles, or the bony "bumps" at the end of the bone at the knee is approximately 15 degrees. Greater or less than normal ranges contribute to a greater torsion angle. So what does this mean? This means that when a person with "normal" ranges of femoral torsion stand, the head of the femur sits itself in a "neutral" position with the least amount of stress on the joint, and toes point in a relatively straight position. Someone with greater than normal torsion angles can either stand with toes out (retroversion) as the "neutral position" to seat the head of the femur correctly, or conversely toes in (anteversion). Greater amount of stretching will not change these inherent angles, and appreciating what you have, and not forcing your motion, is recommended.
Just as the PAO is a mouthful of medical terminology, so is the DFO. Neither the PAO or DFO are procedures to laugh about. Both require time and patience throughout the entire process, and thorough diagnosing for assessing if and how if either procedure is for you.
WHAT IS A DFO?
What exactly is a DFO? Why haven't I heard of it before? Why is it recommended for me? In discussing previous procedures, a hip scope alone helps to address bony anatomy issues affecting the joint and fixing the labrum within the joint. The PAO addresses anatomical issues related to poor depth, or formation, of the acetabulum called hip dysplasia. This issue causes an instability within the joint contributing a different presentation of damage within the joint contributing to pain and dysfunction. This was discussed in previous hip pearls. The DFO is a procedure to address the anatomical issues related to the orientation of the femur to the hip socket. In my experience, the number of orthopedists who look for either or both dysplasia and femoral torsion are increasing whereas in the past, these were not as well identified as to how these effected the joint and damage related to labral or cartilage tears. In addition, these are typically not diagnoses which PCPs will be looking for upon an assessment. The hip world continues to change and evolve rapidly, and these statements will hopefully be too old before too long!
Why does this matter? The orientation of the angle of the neck of the femur at the top of the bone compared to the condyles, or the bony "bumps" at the end of the bone at the knee is approximately 15 degrees. Greater or less than normal ranges contribute to a greater torsion angle. So what does this mean? This means that when a person with "normal" ranges of femoral torsion stand, the head of the femur sits itself in a "neutral" position with the least amount of stress on the joint, and toes point in a relatively straight position. Someone with greater than normal torsion angles can either stand with toes out (retroversion) as the "neutral position" to seat the head of the femur correctly, or conversely toes in (anteversion). Greater amount of stretching will not change these inherent angles, and appreciating what you have, and not forcing your motion, is recommended.
|
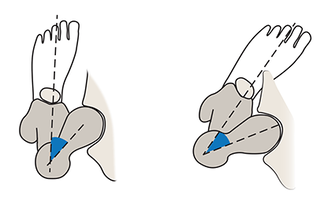
RETROVERSION: This is a less than normal angulation of the neck of the femur to the end of the femur bone. When this is present, the head of the femur must go into external, or outward, rotation in order to achieve "neutral" position with movement. This person will likely be able to sit more comfortably in "criss cross applesauce" positions, and favor a toe out position in standing. ANTEVERSION: This is a greater than normal angulation of the neck of the femur to the end of the femur bone. When this is present, the head of the femur must go into internal, or inward, rotation in order to achieve "neutral" position with movement. This person likely favored the "W" position at a younger age, or perhaps still does. |
|
CONSERVATIVE CARE AND FEMORAL TORSION:
While this Hip Pearl will not get into the actual numbers and measurements to discuss if surgery is an option, it is to help educate why femoral torsion is important in hip health. Knowing this information and trying to address things conservatively, working with your "neutral" position, is important. Many physical therapists will focus on "neutral knee/foot position" and many times this is relatively straight. This position may not apply to you. If someone has severe anteversion, toe in position or "knocked knee" position, the traditional "neutral position" of the lower extremity with single leg squats, for example, will be toward the end of someone's range and difficult to increase strength and/or balance due to the insufficient seated position of the head of the femur in the joint. Your physical therapist can perform relatively easy tests to help identify where your "neutral" hip position is and work within this. It is common for femoral torsion to be an underlying factor with persisting patellofemoral pain (knee pain) or ankle/foot pain, not just pain at the hip. Commonly, the hip will be an area addressed for strength related to knee and ankle pain/issues, especially if there is no mechanism of injury to related to these problems. It has been my experience that strength gains may be challenging for someone with high femoral torsion angles based on how the anatomy interfaces at the hip and the ability for muscles to activate.
While this Hip Pearl will not get into the actual numbers and measurements to discuss if surgery is an option, it is to help educate why femoral torsion is important in hip health. Knowing this information and trying to address things conservatively, working with your "neutral" position, is important. Many physical therapists will focus on "neutral knee/foot position" and many times this is relatively straight. This position may not apply to you. If someone has severe anteversion, toe in position or "knocked knee" position, the traditional "neutral position" of the lower extremity with single leg squats, for example, will be toward the end of someone's range and difficult to increase strength and/or balance due to the insufficient seated position of the head of the femur in the joint. Your physical therapist can perform relatively easy tests to help identify where your "neutral" hip position is and work within this. It is common for femoral torsion to be an underlying factor with persisting patellofemoral pain (knee pain) or ankle/foot pain, not just pain at the hip. Commonly, the hip will be an area addressed for strength related to knee and ankle pain/issues, especially if there is no mechanism of injury to related to these problems. It has been my experience that strength gains may be challenging for someone with high femoral torsion angles based on how the anatomy interfaces at the hip and the ability for muscles to activate.