
Hip Clinical Pearls: #1
|

|
|
Clinical Pearl 1: Intro and Hip Anatomy
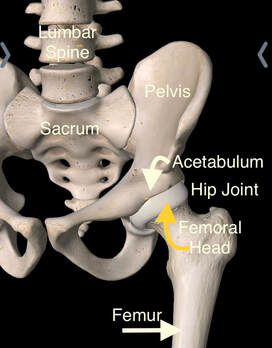
On multiple occasions over the years, I’ve been asked to share general information to help people through injuries, and especially hip related issues. As a professional Physical Therapist, I have been focusing on the hip and pelvis for many years. Research and publications in physical therapy, centered on this region, are not nearly as prevalent as other joints of the body. As a patient, finding detailed information related to hip pain, injury, and interventions including surgery and outcomes, can be a bit challenging. My goal is to cover multiple areas through “clinical pearls”, and share my experience, education, and insights in a similar manner, as if we were in a clinical setting. Picture yourself in an office, or treatment room, with me in front of you, addressing some of your questions, passing along these tidbits of information. This will not be a scientific based, research quoting site, but one to educate and enable you to comprehend more. A LITTLE PERSONAL HISTORY TO SHARE... Since I graduated PT school in the late 1990s, a couple of historical hip related bullets come to mind. First, the primary hip procedure discussed at that time was the total hip arthroplasty or total hip replacement. Fast forward twenty years, and we now have various hip surgical options such as: the hip arthroscopy, Periacetabular Osteotomy, and a hemiarthroplasty to name a few. Second, while participating in gross anatomy class, we were not taught about the labrum within the hip joint. It was, as if, it didn’t exist, and then miraculously showed up after the millennium. Not only did I learn years later that a labrum resides in the hip joint, but that it has a specific function that can be interrupted with injury, and can cause pain and other issues over time. Since the late 90s, the number of reference articles noting that there has been over 600 times, or more, increase in hip surgeries performed, especially for labral repairs, is pretty outstanding! This has obviously been a huge area of growth in Sports Medicine with very specific training for physicians. When I first started hearing of patients undergoing hip scopes, it seemed that physicians took a weekend course and began doing these new procedures. Looking back, I know this was not the case! Post hip arthroscopy referrals would be received from a physician I only understood to be a knee or shoulder specialist, and wondered, “When did he start doing hips? What’s the rehab protocol? Oh, you mean, there is no protocol? Huh.” As the practicing PT, the inference was simply to not screw up the surgical procedure. Since I really didn’t have an appreciation of what was done in the operating room, all I could think was, “Well, that’s GREAT”. Thank goodness, continuing education and PT school now includes this information that has been studied over the past 20 plus years. During my career, of more than two decades, I have learned various things through experience and research, which I will share with you. ANATOMY: First, let’s talk about the basics of anatomy and how the hip joint functions. With regards to anatomy, to put it simply, the hip joint consists of the acetabulum, or concave part of the joint, which lies within the pelvis, and the head of the femur, or convex part of the joint, which sits at the top of the femur or thigh bone. More commonly, the hip is understood to be a “ball and socket” joint. In addition, we have two different types of cartilage in the hip. The labrum is located on the outskirts of the acetabulum, on the pelvic side of the joint, and helps provide greater stability with the joint, acting as a gasket to seal the joint. Articular cartilage lines the acetabulum and femoral head, to allow for smooth joint motion and shock absorption. Articular cartilage can be found in all joints in the body. Furthermore, multiple ligaments are involved in stabilizing the hip joint, and can be found surrounding the innermost bony aspects. Numerous, deep and superficial muscles encircle the hip and facilitate movement. And finally, a handful of nerves, provide both motor and sensory functions to the hip joint, the labrum, and surrounding musculature. There you have it, hip anatomy in a nutshell. In the next clinical pearl, I will address the differences between how your hip joint functions in a weighted and unweighted position. |


1990s option for hip surgery.


|